The diagnosis of Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) relies on an adequate assessment of a hyponatremic state (that is a serum sodium level <136 mmol/l) and on the exclusion of other causative conditions leading to an adequate secretion of antidiuretic hormone (ADH).
Is SIADH serious?
In severe cases, SIADH can cause confusion, seizures, and coma. Treatment usually begins with limiting fluid intake to prevent further buildup. Additional treatment will depend on the cause. Another name for the syndrome is “ectopic ADH secretion.”
What is a common cause of SIADH?
SIADH tends to occur in people with heart failure or people with a diseased hypothalamus (the part of the brain that works directly with the pituitary gland to produce hormones). In other cases, a certain cancer (elsewhere in the body) may produce the antidiuretic hormone, especially certain lung cancers.
Can SIADH be cured?
SIADH should be treated to cure symptoms. While this is undisputed in the presence of grave or advanced symptoms, the clinical role and the indications for treatment in the presence of mild to moderate symptoms are currently unclear.How do you diagnose SIADH?
How is SIADH diagnosed? In addition to a complete medical history and physical examination, your child’s doctor will order blood tests to measure sodium, potassium chloride levels, and osmolality (concentration of solution in the blood). These tests are necessary to confirm a diagnosis of SIADH.
Is SIADH permanent?
The syndrome of inappropriate antidiuretic hormone secretion (SIADH) can occur following traumatic brain injury (TBI), but is usually transient. There are very few case reports describing chronic SIADH and all resolved within 12 months, except for one case complicated by meningo-encephalitis.
What happens if SIADH is untreated?
Symptoms tend to be mild at first and include cramps, muscle weakness, loss of appetite, irritability, and nausea and vomiting. The symptoms continue to become more serious if the SIADH goes untreated and include confusion, hallucinations, seizures and even coma.
Can SIADH cause pain?
SIADH can also arise postoperatively from stress, pain, and medications used. However, not all hospital-acquired hyponatremia is SIADH and SIADH should be differentiated from the hyponatremia that occurs in patients with limited capacity to excrete free water, such as those with chronic kidney disease.How long does it take for SIADH to resolve?
Once the drug is initiated, the patient can be discharged in 24-48 hours if neurological symptoms have resolved or the patient was asymptomatic at presentation. If the underlying cause of SIADH has resolved, the drug can be withdrawn after 2-4 weeks, while carefully monitoring serum Na+ daily for the next 5 days.
What are the complications of SIADH?- Headaches.
- Depression.
- Memory problems.
- Muscle cramps.
- Tremors.
Who is at risk for SIADH?
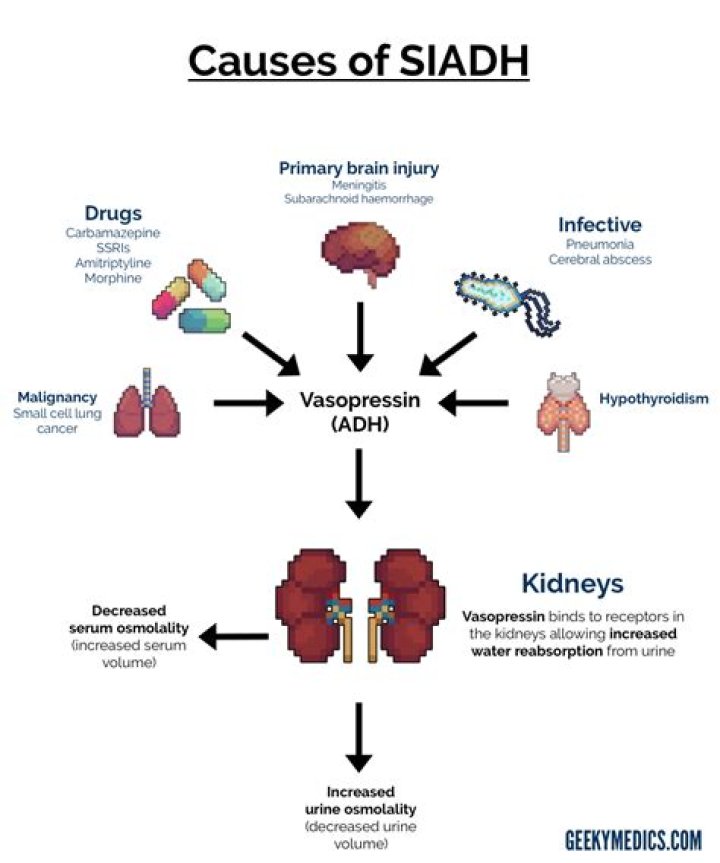
Causes of SIADH Many conditions increase the risk of developing SIADH. SIADH may result when vasopressin is produced outside the pituitary gland, as occurs in some lung and other cancers. SIADH is common among older people and is fairly common among people who are hospitalized.
Why do you get hyponatremia with SIADH?
The syndrome of inappropriate secretion of antidiuretic hormone (SIADH) is a disorder of impaired water excretion caused by the inability to suppress the secretion of antidiuretic hormone (ADH) [1]. If water intake exceeds the reduced urine output, the ensuing water retention leads to the development of hyponatremia.
Is urine sodium high or low in SIADH?
With SIADH (and salt-wasting syndrome), the urine sodium is greater than 20-40 mEq/L. With hypovolemia, the urine sodium typically measures less than 25 mEq/L. However, if sodium intake in a patient with SIADH (or salt-wasting) happens to be low, then urine sodium may fall below 25 mEq/L.
What is used to treat Siadh?
Immediate treatment of the symptomatic patient with SIADH includes intravenous furosemide and 3% sodium chloride injection to produce a negative free-water balance. If the underlying cause of SIADH cannot be corrected, the treatment of choice for chronic SIADH is fluid restriction.
What fluids do you give for SIADH?
Therapeutic modalities include nonspecific measures and means (fluid restriction, hypertonic saline, urea, demeclocycline), with fluid restriction and hypertonic saline commonly used. Recently vasopressin receptor antagonists, called vaptans, have been introduced as specific and direct therapy of SIADH.
Can a person recover from low sodium levels?
Hyponatremia can result from multiple diseases that often are affecting the lungs, liver or brain, heart problems like congestive heart failure, or medications. Most people recover fully with their doctor’s help.
Is SIADH genetic?
Hereditary SIADH: A gain of function mutation in the gene for the renal V2 receptors (located on the X chromosome) is responsible for hereditary SIADH.
Why is urine concentrated in SIADH?
With SIADH, the urine is very concentrated. Not enough water is excreted and there is too much water in the blood. This dilutes many substances in the blood such as sodium. A low blood sodium level is the most common cause of symptoms of too much ADH.
What is the fluid limit for SIADH?
9 Otherwise, fluid restriction (less than 1 to 1.5 L per day) is the mainstay of treatment and the preferred mode of treatment for mild to moderate SIADH. 20 The combination of loop diuretics with a high-sodium diet may be required to achieve an adequate response in patients with chronic SIADH.
Does SIADH cause low urine output?
In SIADH, the body is unable to suppress the secretion of ADH, leading to impaired water excretion and reduced urine output. Normally, when water is ingested, serum tonicity and osmolality decrease and ADH is suppressed, resulting in output of a dilute (less concentrated) urine. This pathway is impaired in SIADH.
Can drinking too much water cause hyponatremia?
Drinking excessive amounts of water can cause low sodium by overwhelming the kidneys’ ability to excrete water. Because you lose sodium through sweat, drinking too much water during endurance activities, such as marathons and triathlons, can also dilute the sodium content of your blood.
How does SIADH affect blood pressure?
In SIADH the blood pressure is normal and there is no edema. In contrast in the hyponatremia of liver cirrhosis and heart failure the plasma measurements indicated are usually slightly elevated, the blood pressure is low and there is edema. The typical patient with hypernatremia is old and has no thirst sensation.
What is the difference between Siadh and hyponatremia?
In SIADH, hyponatremia is caused by water retention due to inappropriate secretion of antidiuretic hormone (ADH) (10-15). But in CSWS, hyponatremia is associated with high urine output, high urine sodium concentration, and plasma volume depletion (16).
How does Siadh cause pneumonia?
The pathogenesis for the development of SIADH in COVID-19 pneumonia per preliminary reports is due to the production of certain proinflammatory cytokines, particularly, IL-6.
Is SIADH the same as diabetes insipidus?
Impaired AVP secretion or response results in impaired renal concentration and is termed diabetes insipidus (DI). Hyponatremia that results from AVP production in the absence of an osmotic or hemodynamic stimulus is termed syndrome of inappropriate antidiuretic hormone secretion (SIADH).
Which drug is approved for treatment of hyponatremia due to syndrome of inappropriate ADH secretion?
Conivaptan and tolvaptan are currently the only vasopressin receptor antagonists that are commercially available in the United States and FDA-approved for the treatment of euvolemic hyponatremia in hospitalized patients.
