A retrospective payment system gives providers greater influence over payment rates than they generally have under PPS. … The use of prospective payment leads to more predictable payment levels for payers, patients, and providers and is typically associated with simpler administrative systems.
What is retrospective payment?
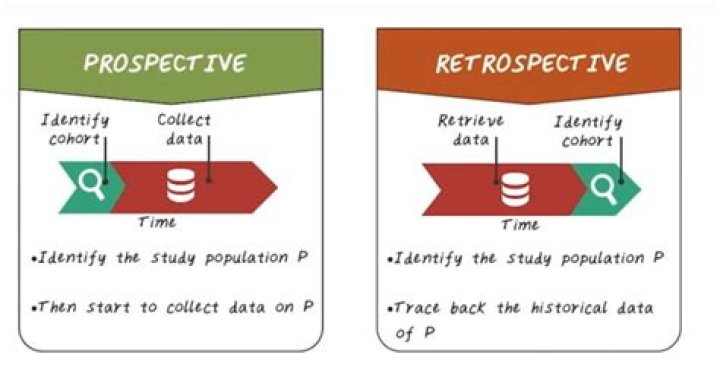
(ret’rō-spek’tiv pā’mĕnt) A payment made after an action has happened or therapy provided such as in fee-for-service reimbursement.
Why are prospective payment systems different?
Although the PPS payment system may sound somewhat like a health maintenance organization (HMO), there are differences. Instead of a monthly payment amount for all services, like an HMO provides, PPS provides the healthcare facility with a single predetermined payment for each Medicare patient.
What is retrospective payment in healthcare?
Retrospective payment plans pay healthcare providers based on their actual charges. With a retrospective payment plan, a provider will treat a patient and submit an itemized bill to an insurance company detailing the services rendered.Which term is an example of prospective payment?
A Prospective Payment System (PPS) is a method of reimbursement in which Medicare payment is made based on a predetermined, fixed amount. The payment amount for a particular service is derived based on the classification system of that service (for example, diagnosis-related groups for inpatient hospital services).
What is a non prospective payment system?
providers are limited on the fixed amount and only allow for those fixed systems of care to. code/bill for. Non-Prospective Payments, also called Retrospective payments, is a reimbursement method that. pays providers on actual charges (Prospective Payment Plan vs.
What are the benefits of a prospective payment system for the payer?
One important advantage of Prospective Payment is the fact that code-based reimbursement creates incentives for more accurate coding and billing. PPS results in better information about what payers are purchasing and this information can be used, in turn, for network development, medical management, and contracting.
What are the classification systems used with prospective payments?
The Ambulatory Patient Groups (APGs) are a patient classification system that was developed to be used as the basis of a prospective payment system (PPS) for the facility cost of outpatient care.How do the prospective payment systems impact operations?
The prospective payment system rewards proactive and preventive care. … The prospective payment system stresses team-based care and may pay for coordination of care. These value-based care models promote doctors, hospitals, and other providers to work together to receive value-based reimbursements from CMS.
What is prospective model?Prospective IE models combine central features of the established IE methods into a new framework. They allow researchers to conduct comprehensive and dynamic scenario analyses of society’s future metabolism and to study the potential system-wide effect of sustainable development strategies.
Article first time published onIs prospective payment system good or bad?
PPS proved effective at curbing cost growth. However, because it contained incentives for hospitals to shorten stays and to choose the least expensive methods of care, PPS raised concerns about possible declines in the quality of care for hospitalized Medicare patients.
Why did Medicare move to a prospective payment system?
The change from cost-based reimbursement to prospective payment represents a fundamental change in the role of the Medicare program within the health care system. … The new payment system is designed to change hospital behavior by directly altering the economic incentives facing hospital decisionmakers.
Why was the prospective payment system established?
The Medicare Inpatient Prospective Payment System ( IPPS ) was introduced by the federal government in October, 1983, as a way to change hospital behavior through financial incentives that encourage more cost-efficient management of medical care.
What is the difference between APC and DRG?
APCs are similar to DRGs. Both APCs and DRGs cover only the hospital fees, and not the professional fees, associated with a hospital outpatient visit or inpatient stay. DRGs have 497 groups, and APCs have 346 groups. … Only one DRG is assigned per admission, while APCs assign one or more APCs per visit.
What is the outpatient prospective payment system?
The Outpatient Prospective Payment System (OPPS) is the system through which Medicare decides how much money a hospital or community mental health center will get for outpatient care to patients with Medicare. The rate of reimbursement varies with the location of the hospital or clinic.
In what way did retrospective reimbursement contain perverse financial incentives?
In what way did retrospective reimbursement contain perverse financial incentives? In retrospective reimbursement, the amount of reimbursement is established after evaluating the costs retrospectively. … There was no incentive to control costs because providers could increase their profits by increasing costs.
How the prospective payment system for inpatient care affected a hospital financially?
Under this system, hospitals were paid whatever they spent; there was little incentive to control costs, because higher costs brought about higher levels of reimbursement. Partly as a result of this system of incentives, hospital costs increased at a rate much higher than the overall rate of inflation.
Which act resulted in a prospective payment system PPS that issues a predetermined payment for inpatient services?
TEFRA also enacted a prospective payment system (PPS), which issues a predetermined payment for inpatient services. Previously, reimbursement was generated on a per diem basis, which issued payment based on daily rates.
How are the Medicare prospective payment system and the use of capitated rates in managed care organizations similar How are they different?
Medicaid’s Blended System Capitation incentivizes preventive health care, including in-home services, while the limited FFS treatments allow for cost analysis and adjustments between doctors, service providers, and Medicaid.
Under which prospective payment system are facilities reimbursed for the provision of outpatient procedures?
Ambulatory Payment Classification (APC) System: An encounter-based classification system for outpatient reimbursement, including hospital-based clinics, emergency departments, observation, and ambulatory surgery. Payment rates are based on categories of services that are similar in cost and resource utilization.
What is the difference between fee for service and diagnosis related group prospective payments?
Milton Roemer, Hospital Bed Supply and Economics of Health The DRG system was officially adopted in 1983 by the US Health Care Financing Administration (HCFA) as the basis for payment for hospitalization of Medicare patients.
What is Skilled Nursing Facility Prospective Payment System?
The Medicare Patient-Driven Payment Model (PDPM) is a major overhaul to the current skilled nursing facility (SNF) prospective payment system (PPS). It is designed to address concerns that a payment system based on the volume of services provided creates inappropriate financial incentives.
What are the primary methods of payment used for reimbursing providers by Medicare and Medicaid?
The three primary fee-for-service methods of reimbursement are cost based, charge based, and prospective payment. Under cost-based reimbursement, the payer agrees to reimburse the provider for the costs incurred in providing services to the insured population.
When and how is a fee-for-service paid?
Fee-for-service is a system of health insurance payment in which a doctor or other health care provider is paid a fee for each particular service rendered, essentially rewarding medical providers for volume and quantity of services provided, regardless of the outcome.
What is the incentive under fee-for-service reimbursement?
Fee-for-service (FFS) is a payment model where services are unbundled and paid for separately. In health care, it gives an incentive for physicians to provide more treatments because payment is dependent on the quantity of care, rather than quality of care.
When was the prospective payment system established?
The PPS was established by the Centers for Medicare and Medicaid Services (CMS), as a result of the Social Security Amendments Act of 1983, specifically to address expensive hospital care. Regardless of services provided, payment was of an established fee.
What are the pros and cons of DRG?
The advantages of the DRG payment system are reflected in the increased efficiency and transparency and reduced average length of stay. The disadvantage of DRG is creating financial incentives toward earlier hospital discharges. Occasionally, such polices are not in full accordance with the clinical benefit priorities.
What is included in a DRG payment?
In general, a DRG payment covers all charges associated with an inpatient stay from the time of admission to discharge. The DRG includes any services performed by an outside provider. Claims for the inpatient stay are submitted and processed for payment only upon discharge.
What is difference between a DRG and a MS DRG?
In 1987, the DRG system split to become the All-Patient DRG (AP-DRG) system which incorporates billing for non-Medicare patients, and the (MS-DRG) system which sets billing for Medicare patients. The MS-DRG is the most-widely used system today because of the growing numbers of Medicare patients.
